 Home
Home

 Artists
Artists
 Search
Search
 Recent
Recent
 Random
Random
 Posts
Posts
 DMs
DMs
 Tags
Tags
 Random
Random
 Importer
Importer
 Import
Import
 FAQ
FAQ
 Account
Account
 Register
Register
 Favorites
Favorites
 Login
Login

Eating Less Protein won't make you Live Longer (Patreon)
Downloads
Content
There is this idea floating around that eating less protein will make you live longer. I talked about this very briefly in another post but let’s dig deeper. Many of y’all who got to the poll at the end of the post seemed to be aware of low-protein for longevity idea:
<figure>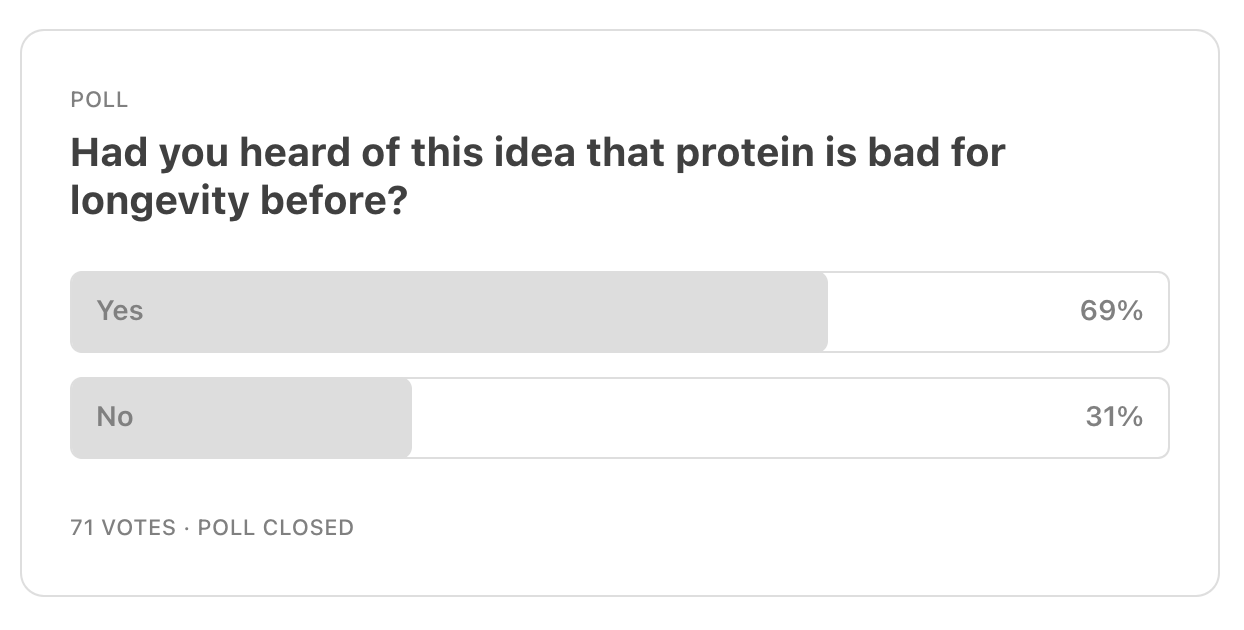 </figure>
</figure>In fact, this was something I was trying to puzzle out in my head about 5+ years back when I saw this lecture of Ron Rosedale’s titled The Intimate Connection Between Cancer, Aging, Protein, and TOR. He presented an interesting story for why what builds you up and repairs your body won’t necessarily make you live longer. That is, once you have carried out nature’s imperative of reproducing, nature doesn’t really care about you and isn’t interested in making you live forever.
<figure> </figure>
</figure>In fact, I talk about this concept of there seeming to be a trade-off between growth and longevity in my fasting video from January just this year. I explain that there is some evidence that reducing the activation of certain growth factors seems to be good for longevity. However, as we’ll explore in this article, I think there is a big difference between constant reduction of growth factors and temporary reductions of growth factors.
Why do people say eating less protein increases your lifespan?
<figure> </figure>
</figure>David Sinclair has become very popular for his contributions to longevity research and has been interviewed many times on multiple podcasts as a longevity expert. He’s been on most of the big podcasts like Joe Rogan, Lex Fridman, Andrew Huberman, Peter Attia, Lewis Howes, Tom Bilyeu and several others. In my opinion, David Sinclair has done a lot to popularize this idea that restricting protein is good for longevity.
Bryan Johnson is a rising star in the longevity space. Not as a researcher, but as he calls himself, a ‘rejuvenation athlete.’ He’s spent millions of dollars to try and age very slowly. He takes 100+ pills, eats a specific amount of calories per day, has a specific exercise routine, sleep routine, does various skin treatments, has a device exercising his pelvic floor so he doesn’t have to get up and pee at night, and is constantly monitoring blood markers, organ health, getting scans of his skin et cetera. He apparently has a team of 20+ doctors working with him on this.
<figure> </figure>
</figure>Taking a look at his protocol, it looks quite influenced by ideas that David Sinclair promotes. For example, he’s on a strict vegan diet (except he does take collagen) and considering you need more protein as you age, the diet’s protein is on the lower end in my opinion but much better than the RDA of 0.8kg/kg.
He said that he’s upped his calorie intake because he was looking too gaunt. Where it was about 1980 calories before, per his recently updated daily protocol, his daily intake is now set at a strict 2250 calories. This is still a caloric deficit for his physique, but less so than before. He tries to compensate for the testosterone reduction due to calorie restriction with testosterone patches.
<figure> </figure>
</figure>His 2250 calories have a spread of 17% protein, 35% carbs, and 48% fat which puts him at about 96 grams of protein per day. Considering he currently weighs 163 pounds or about 74 kilograms, that puts him at 1.3g/kg total protein. Recent research suggests that we want to be getting at least 1.2g/kg to 1.6g/kg of protein, so Johnson’s protein intake isn’t bad but we’ll get into protein quality and amino acid spread later on.
One tangent I’ll add here is that there are several animal studies suggesting longer lifespans from lower protein or very calorie restricted diets, but that’s not always the result. Here’s a snippet from anti-aging scientist Dr. Matt Kaeberlein on Peter Attia’s podcast talking about a particular mouse study:
Kaeberlein: "It wasn't the case that the diets that were energetically lowest gave the longest lifespan as you might expect from caloric restriction, the diet that gave the absolute longest lifespan had something like 40% protein in it…”Attia: “And how calorie restricted was that?”Kaeberlein: “They were not calorically restricted at all.”Attia: “So you’re saying that a diet that was ad libitum with 40% protein that had the best outcome?”Kaeberlein: “The best absolute lifespan, yes.”
They say the issue with protein is mTOR
David Sinclair says “there is a mechanism called mTOR that responds to certain amino acids that are found in more abundance in meat … and when it responds it actually shortens lifespan.”
“just like testosterone and growth hormone you will get temporary-, maybe not temporary-, immediate health benefits. You’ll feel great, you’ll get more muscle, energy. But the problem is, I think it’s at the expense of long-term health and longevity.”
I have an issue with this concept of natural whole-foods making you feel great now being somehow bad for you later.
Reminds me of stories of doctors warning patients against their keto or carnivore diet even though it reversed so many issues for them:
‘Sure, your meat and animal-food heavy diet may have reversed your prediabetes, had you lose 40 lbs, gain tons of muscle, reduced your fasting insulin, blood sugar and triglycerides and increased testosterone, and you may have great libido, mood and energy levels… but this is going to be bad for you in the long run.’
David Sinclair says here that "through a lack of amino acids, particularly three of them, leucine, isoleucine and valine, the body will down-regulate mTOR.”
In this article we’ll cover:
1. Why lowering mTOR doesn’t make sense: What are you going to eat?
2. Exercise less and you’ll live longer?
3. Do frail people live longer?
4. What if you need to do more mTOR activating things?
5. Is Protein really causing Cancer?
- - - - -
1. Why lowering mTOR doesn’t make sense: What are you going to eat?
<figure> </figure>
</figure>In a long video titled Meat vs. Plants for Longevity, Dr. Paul Saladino digs up a paper titled The actions of exogenous leucine on mTOR signalling and amino acid transporters in human myotubes. To David Sinclair’s point, the paper demonstrates that leucine is indeed an activator of mTOR. However, if you scroll down to Figure 2, you’ll see that insulin activates mTOR at least as much as leucine.
<figure>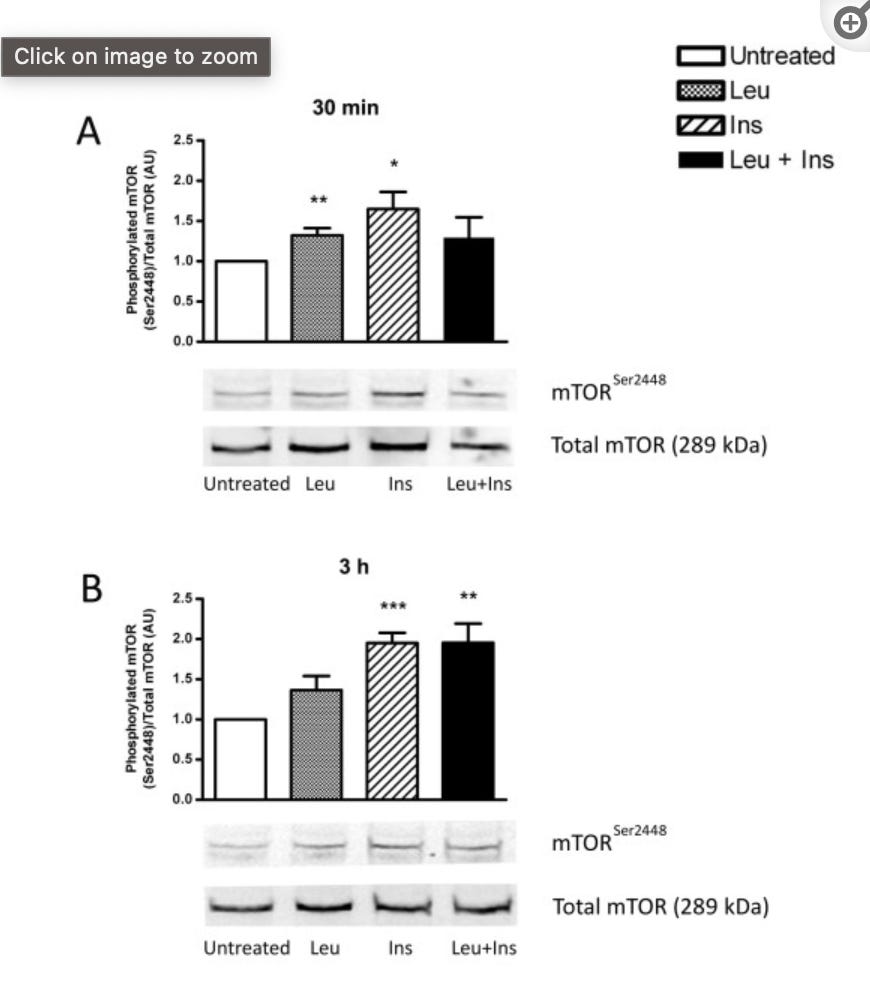 </figure>
</figure>This study has a nice visual representation of insulin’s activating of mTOR, but this isn’t just tucked away in one study. Insulin activating mTOR is a well known phenomenon.(S)
Paul makes a good point: If you’re going to avoid getting protein because of mTOR, what are you going to eat? Insulin, which is triggered by eating carbohydrates, triggers mTOR too. So are we to restrict protein and carbohydrate?
<figure> </figure><figure>
</figure><figure>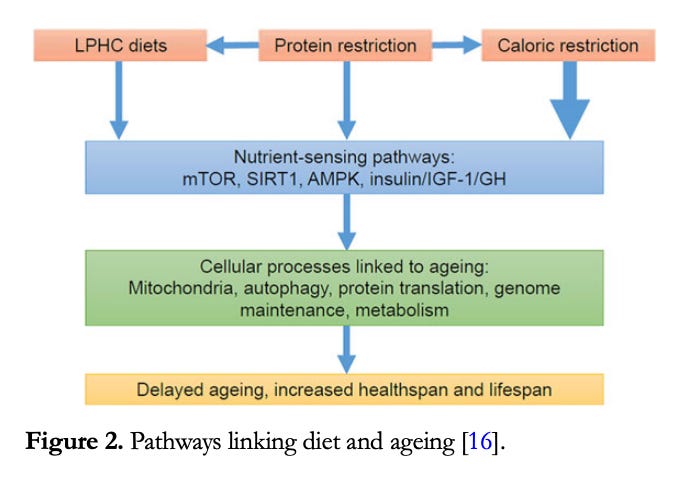 </figure>
</figure>A 2016 paper pointed to the Okinawans as an example of a people that live very long thanks to their diet that prioritizes carbohydrate over protein. However, as I explain in this video of mine here, the idea that the Okinawans were living longer from eating mostly purple sweet potatoes is based on a majorly flawed 1949 data point from right after the war when Okinawans were starving and the only thing they had available to eat was sweet potatoes.
<figure> </figure>
</figure>A much more appropriate study of the Japanese elderly’s diet suggests the complete opposite of the BBC Headline A high-carb diet may explain why Okinawans live so long resulting from that 2016 paper. It suggests those that lived the longest ate more animal protein and less carbohydrate.
1. Nutrient intakes in 94 Japanese centenarians investigated between 1972 and 1973 showed a higher proportion of animal protein to total proteins than in contemporary average Japanese.
2. High intakes of milk and fats and oils had favorable effects on 10-year (1976-1986) survivorship in 422 urban residents aged 69-71. The survivors revealed a longitudinal increase in intakes of animal foods such as eggs, milk, fish and meat over the 10 years.
3. Nutrient intakes were compared, based on 24-hour dietary records, between a sample from Okinawa Prefecture where life expectancies at birth and 65 were the longest in Japan, and a sample from Akita Prefecture where the life expectancies were much shorter. Intakes of Ca, Fe, vitamins A, B1, B2, C, and the proportion of energy from proteins and fats were significantly higher in the former than in the latter. Intakes of carbohydrates and NaCl were lower.
2. Exercise less …and you’ll live longer?
<figure> </figure>
</figure>If lowering mTOR would make us live longer, we should then do something that makes no sense: exercise less. Exercise is well known to stimulate mTOR, and the increase in muscle size and strength that we experience from resistance exercise is due to mTOR activation.(S)
Further, according to mTOR and the health benefits of exercise, the other health benefits we experience from exercise are thanks to mTOR
Many of the health benefits of exercise are mediated by the mammalian/mechanistic target of rapamycin (mTOR), either in complex 1 or 2, not only within the working muscle, but also in distant tissues such as fat, liver, and brain.
Cognitive decline is another huge worry in the aging elderly population and it’s well known that exercise can provide resistance against cognitive decline. Per a 2017 paper in Behavioral Brain Research, because “mTOR has been implicated in enhancing learning and memory as well as antidepressant effects,” and “exercise increased p-mTOR-positive neurons in the medial prefrontal cortex, striatum, hippocampus, hypothalamus, and amygdala” in rats, they surmise that “increases in mTOR signaling could contribute to the beneficial effects of exercise on cognitive function and mental health.”
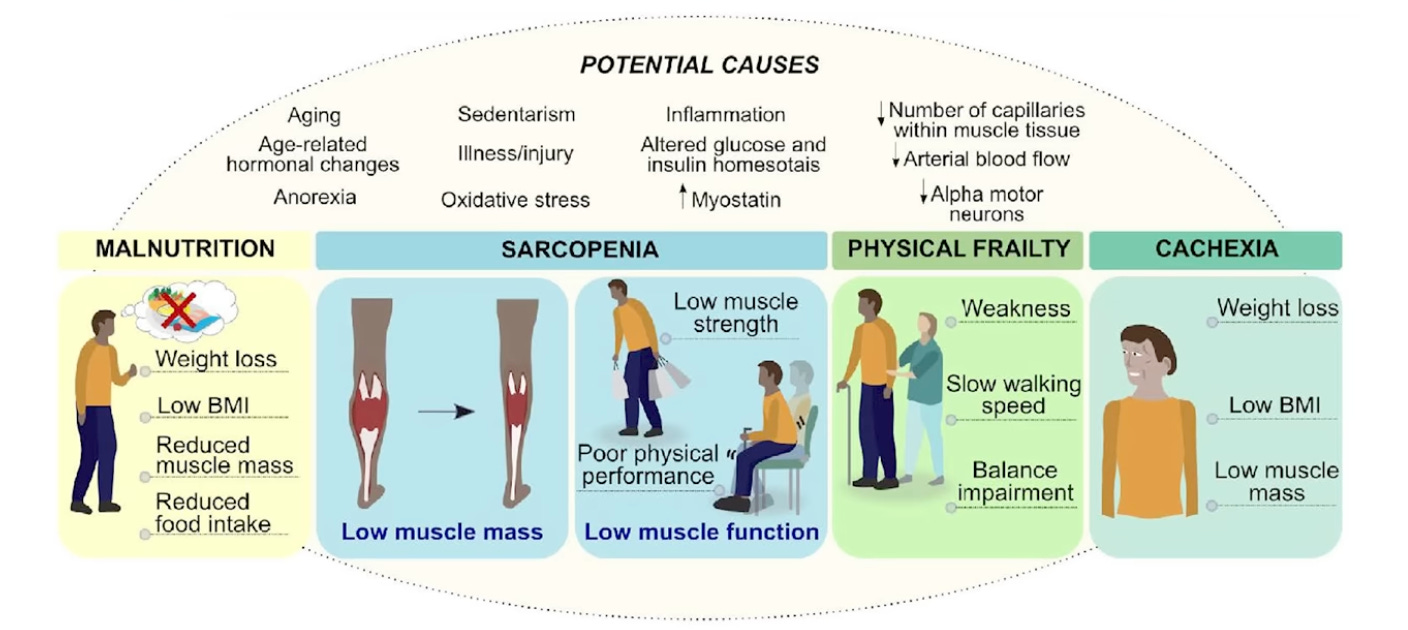
3. Do frail people live longer?
<figure> </figure>
</figure>As discussed in my three previous posts about protein (1,2,3), having plenty of muscle and ample protein intake is fantastic insurance against metabolic disease, obesity, diabetes and cognitive decline. Further, it’s known that having more muscle mass generally makes people live longer.
Per Muscle Mass Index As a Predictor of Longevity in Older Adults,
This study establishes the independent survival prediction ability of muscle mass as measured by bioelectrical impedance in older adults, using data from a large, nationally representative cohort. This is in sharp contrast to BMI, whose association with mortality in older adults is inconsistent, at best.
Again, we need mTOR to stimulate the growth of muscle. As this 2015 paper puts it:
“signaling by mTOR is necessary for an increase in protein synthesis and the hypertrophy that occurs in response to increased mechanical loading.”
Further, the amino acid that we’re supposed to avoid to avoid mTOR activation and supposedly live longer, leucine, is key in inducing muscle protein synthesis. In my video Protein is not protein, I mention Dr. Layne Norton who did his PhD dissertation on the critical role of leucine in building muscle.
The paper Optimizing Adult Protein Intake During Catabolic Health Conditions says:
“Leucine provides an important example of an essential amino acid where the RDA of 42mg/kg body weight is significantly less than the 100-110 mg/kg required to optimize metabolic regulation and skeletal muscle protein synthesis.”
100mg per kilogram bodyweight would mean that a 75kg or 165lb pound man needs to get 7500 milligrams of leucine per day to maintain healthy muscle … but this is the specific amino acid we should avoid to reduce mTOR activation and live longer?
<figure> </figure>
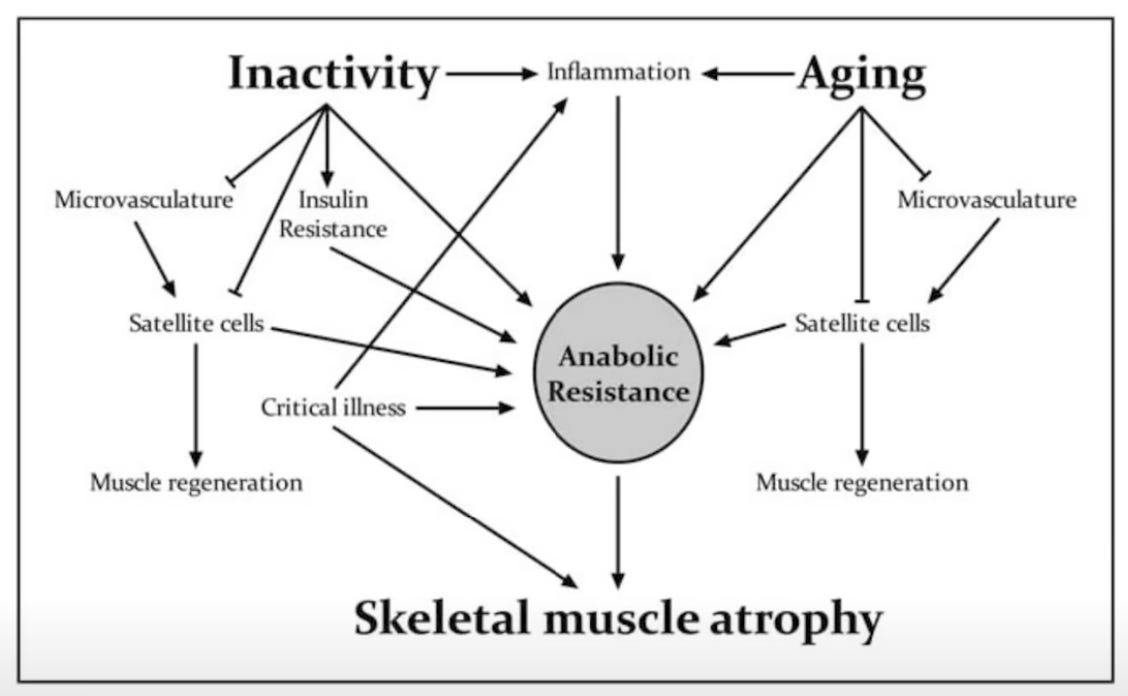
</figure>4. You need to do more things that activate mTOR as you age
<figure>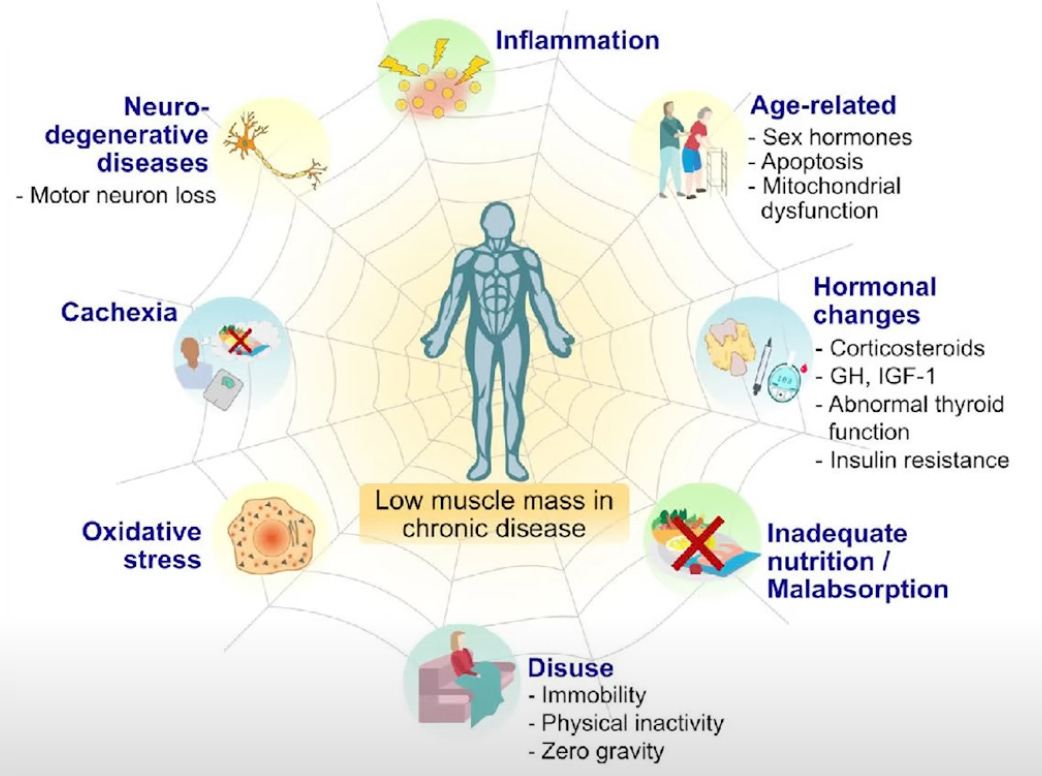 </figure>
</figure>What makes this all even more ironic is that the body develops anabolic resistance as we age. Simply put, elderly people have to try harder to maintain their muscle. They require more leucine, protein and exercise because their muscles are resistant to the stimulating effects of these.
“Periodic activity, even in small quantities, and protein supplementation may serve as effective strategies to offset the loss of muscle mass with aging, specifically during periods of inactivity.”
-The Impact of Step Reduction on Muscle Health in Aging: Protein and Exercise as Countermeasures
Dr. Stuart Phillips says on Rhonda Patrick’s podcast that elderly people need even more of that mTOR stimulating amino acid, leucine.
"we need more leucine, or more BCAA's or more essential amino acids which translates into you need more protein to trigger the whole turning the protein synthetic process on. … it’s really about the leucine that they consume, particularly for their muscle, that’s important"<figure>
 </figure>
</figure>A paper titled Defining anabolic resistance: implications for delivery of clinical care nutrition recommends that the elderly
"ingest at least 1.2g of protein/kg/day with evenly distributed protein boluses 0.4 g/kg with a recommendation to consume a protein containing meal presleep."
Remember, that 1.2g/kg is a minimum they’re recommending, they didn’t say that that is what’s optimal. They also specifically recommend supplementing the mTOR activating amino acid leucine:
"Fortifying suboptimal protein meals with 3g of leucine is an emerging strategy in older individuals who cannot consume multiple high-protein meals."<figure>
 </figure>
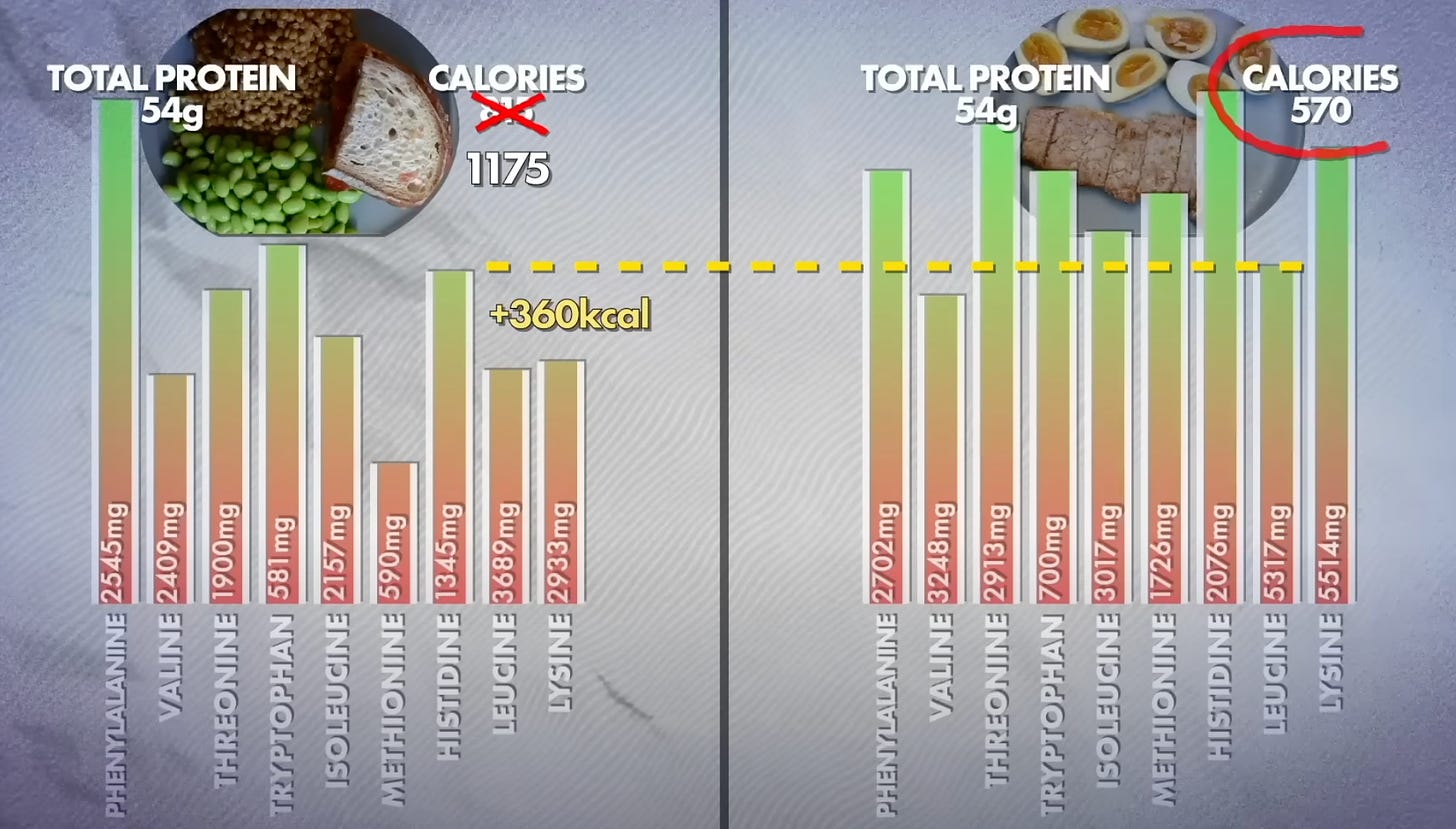
</figure>This is where the importance of protein quality comes in. As discussed in my Protein is not protein video, animal proteins all reach the “high-quality” protein ranking because they provide plenty of each amino acid and are easily digested. Whole plant proteins generally have much lower protein quality scores because they have less of each amino acid in a worse balance and they are less well digested. Further, the elderly experience a decline in stomach acid (hypochlorhydria) which means it is harder for them to digest protein in general.
As I pointed out in that video you’re going to need to eat a lot more calories if you’re getting your protein from whole plant foods. This is a problem not just because your body composition won’t be as good, but it’s well known that elderly people suffer from a decline in appetite, so they have less ability to cram tons of food in there.
<figure> </figure>
</figure>Protein powders may be a good option for the elderly for this reason. Keep in mind you’ll also need to get more pea or soy protein powder than whey to match the leucine and essential amino acid content.
“The scientific report of the Dietary Guidelines Committee for Americans and Canada’s new food guide have endorsed a shift away from animal-protein-based diets, towards a more economically and ecologically sustainable source of protein derived from plants. However, a caveat to this recommendation is that animal-derived protein, such as, dairy, eggs, and meat are high(er) quality protein sources than most plant-based proteins. For example, ingestion of whey protein led to a greater muscle protein synthesis response than wheat protein, in healthy older mean, despite being matched for total protein content.”
-Nutritional supplements to support resistance exercise in countering the sarcopenia of aging
 </figure>
</figure>Unfortunately, protein alone is insufficient to overcome anabolic resistance in the elderly. Ideally, elderly people should be incorporating heavy resistance training as well.
Per Optimizing Adult Protein Intake During Catabolic Health Conditions,
“The age-related reduction in the sensitivity of MPS [Muscle Protein Synthesis] to exercise or protein can be overcome with greater volumes of resistance exercise or greater doses of protein; however, greater exercise volumes may be impractical for many older persons.”
Don’t forget, exercise also activates mTOR.
- - - -
5. No, protein isn’t causing cancer
<figure> </figure>
</figure>“I know David Sinclair has brought up a lot of stuff, saying I really try to limit mTOR and IGF-1 … and it will never cease to amaze me how many scientists do not understand the difference between a short-term, truncated, acute response to a stressor versus dysregulated signaling that persists indefinitely.” -Layne Norton<figure>
 </figure>
</figure>Layne Norton and Peter Attia make some great points in the video Dispelling myths that excess protein intake increases cancer risk | The Peter Attia Drive Podcast
Dr. Norton points out that the kind of mTOR elevations that actually lead to cancer originate at insulin resistance. Insulin resistance is a disease state where mTOR is chronically elevated. Layne says:
“and so it’s like this chronic, low-level pushing of that button. …that is a big difference from a dose of protein that causes mTOR to rise and then go back down in a natural rhythm.”
Chronic elevation of mTOR from a disease state is very different from getting a pulse of mTOR when you have a big protein meal, or when you exercise, or even when you forego a steak and eat sweet potatoes and quinoa.
If you think about this, it really seems that pulses of stressors rather than constant drips of them are better for the human body. For example:
・Plenty of evidence shows that rather than constantly being in the perfect temperature, exposing yourself to a pulse of high heat in the sauna is very good for us.
・Similarly, a pulse of extreme cold in an ice bath confers benefits as well.
・Plenty of studies show that a fasting pattern of ‘feast and fast,’ whether it be intermittent fasting or eating every other day, is better for us than constantly grazing.
 </figure>
</figure>Layne says:
“Where are all the resistance trained people that are getting cancer by the droves? Because if you want to talk about amplitude of response from mTOR, resistance training dwarfs what protein does. If we look at the meta-analyses on cancer incidence amongst resistance trainers, and there's getting to be some now, we see lower levels of cancer in people who resistance train.”
He goes on to re-emphasize that point that there is a huge difference between pulsing mTOR by doing things like eating protein and having mTOR constantly activated via a disease state.
“Most protein in these meta-analyses looking at cancer, I mean ‘high-protein’ is above 70g of protein per day or 1.2g/kg of body weight. Ok, well, most Americans eat high-protein by definition of the RDA [remember the RDA is 0.8g/kg and it is simply the minimum to prevent deficiencies] but where is it from? It’s from burgers and hotdogs, like a bunch of processed meat.”
The point is, these studies claiming high-protein diets cause cancer where they take a bunch of people, ask them what they eat to determine whether they’re eating a ‘high’ protein diet or a ‘low’ protein diet … high-protein usually indicates a low-quality, unhealthy diet. A salad and a ribeye with 52 grams of protein is very different from 52 grams of protein from Big-Macs and fries.
<figure> </figure>
</figure>Hold up, didn’t T. Colin Campbell show that low protein prevents cancer in rats?
T. Colin Campbell, famous for The China Study, which argues that animal protein is terrible for health, has popularized this idea that animal protein causes cancer. Dr. Chris Masterjohn, PhD in Nutritional Sciences, has written a great article on this.
In 1968, “a research paper from India surfaced in an obscure medical journal” showing that aflatoxin only produced liver cancer in rats when they were fed high levels of casein, a milk protein. Campbell was surprised and skeptical, but he attempted to replicate these findings, and thus was born his two-decade research program showing that animal protein, but not plant protein, was the single most important trigger that turns cancer “on” like a light switch.
Note that the study that got Campbell so excited didn’t show that high-casein diets cause liver cancer. They found that administering a liver toxin to rats had different effects depending on the protein levels.
Masterjohn points out that the Indian researchers published two papers. The paper Campbell didn’t mention showed that low-casein diets make aflatoxin much more toxic to rats. They stopped giving the low-protein rats aflatoxin at six months because half of those animals died. Put another way, the low-protein rats didn’t live long enough to get cancer. The high-protein rats did develop cancer from being constantly administered a liver toxin, but they lived longer than the rats on the low protein diet.
Campbell writes himself in his 1972 study that:
“A deficiency of dietary protein was shown to increase the toxicity of aflatoxin for rats.”<figure>
 </figure>
</figure>In his studies on rats on a 5% protein diet versus rats on a 20% protein diet, unsurprisingly, the rats on a 5% protein diet totally failed to grow properly. They only achieved half the normal weight for such a rat. These animals weren’t just small, they were unhealthy, having defunct liver function that resulted in fatty livers. Campbell acknowledged that the protein in the diet was insufficient for developing a healthy liver:
“…the normal rate of cell proliferation would have been decreased during protein deprivation, which is similar to the retardation of brain cell growth of young malnourished animals described by Winick and Rosso (18).”
Here are some more highlights from the distinguished T. Colin Campbell
・In 1978, Campbell was part of a study that found that environmental toxins were even more toxic to rats on a low-protein diet.
・His study from 1980 replicated the finding from the Indian study that protein deprivation made aflatoxin even more toxic to rats’ livers. It was another situation of early death on a low-protein diet or living longer but getting cancer on a high-protein diet.
・Yet another one of his studies from 1989 once again found that low-protein diets are worse for rats enduring the liver toxin, aflatoxin.
The most surprising part of Masterjohn’s article is where he shows that T. Colin Campbell ignored his own data that showed that high-protein diets protect against the initiation of cancer.
<figure> </figure>
</figure>In a 1983 experiment, Campbell’s group fed rats either a 5% or 20% casein diet at the start, during the aflatoxin dosing period. Then, they got either a 5% or 20% casein diet during the 12 weeks after.
What they are watching out for at the start of the experiment is damage indicating the development of cancer, called “pre-cancerous lesions.” Then, in the 12 weeks after that, they are looking for the development of those precancerous lesions. The idea is to see whether these low and high-protein diets are initiating cancer from zero, and/or if they are promoting the development of cancer that is already present.
It turned out that high-protein did in fact slightly worsen cancer if the rats already had it. However, the high-protein diet was powerfully protective against the initiation of cancer. What this would suggest is that if you don’t have cancer, you should eat plenty of protein to protect yourself from it. If you already have cancer, protein might promote the development of the cancer.
Even then, Masterjohn points out that the difference in cancer development between the high-protein rats who already had cancer and the low-protein rats who already had cancer was “not very dramatic.” Nonetheless, Masterjohn has said himself he may consider a low-protein diet if he had cancer, but will eat plenty of protein as long as that is not the case.
Plenty of protein should help make the body robust enough to resist carcinogenic factors that try to make a chink in the armor to initiate the development of cancer. However, once the body enters the disease state of cancer, its utilization of protein may be deranged such that the repairing and growth-promoting effects of protein may be utilized by the cancer to grow itself.
An example of a similar phenomenon is kidney disease. Low-protein diets do in fact confer better outcomes to people with kidney disease. However, as Dr. Stuart Phillips has said, it doesn’t make sense to restrict protein for fear of kidney disease because it is the disease state that is preventing the body from appropriately utilizing the protein, not the other way around. It would be like saying we should avoid water to not get prostate cancer because people with prostate cancer have trouble peeing.
<figure> </figure>
</figure>I’ll cap this discussion off with something Peter Attia said:
“I’m still waiting for somebody to demonstrate for me that if there is an increase in the risk of cancer associated with higher protein intake in humans, I’d like to see that quantified. But, I would like to see somebody demonstrate that if there is an increase in risk - that quantifiable increase in risk, is greater than the offset of sarcopenia [the muscle wasting that occurs as people age] because that’s something for which there is no ambiguity. We have all the data in the world to point to the devastation of sarcopenia on an aging population and we know full well that two things have to be true to avoid sarcopenia: [1] adequate protein intake which, as you age, gets bigger and bigger. That number goes up and up and up due to anabolic resistance … coupled with [2] strength training. Here we have something for which there is no uncertainty. You must consume increasing amounts of protein and you must do strength training to ward off sarcopenia as you age and if you don’t, here is your mortality trajectory: awful. Let’s compare all of that to this questionable risk [of cancer due to consuming excess protein] for which frankly I don’t see data.”